

Introduction
According to the Russian register renal impairment at the time of diagnosis was noted in every fifth patient with multiple myeloma (MM). Timely induction therapy followed by autologous stem cell transplantation (ASCT) in some cases contributes to the reversibility of renal failure. Although ASCT appears safe in patients with mild and moderate renal impairment, there are limited data in those with severe acute kidney injury. These patients are often considered to be unfit for ASCT.
The aim of the study
To study the efficacy and safety of high dose therapy followed by ASCT in patients with MM and renal failure and to evaluate the results of the treatment depending on the severity of acute kidney injury.
Materials and methods
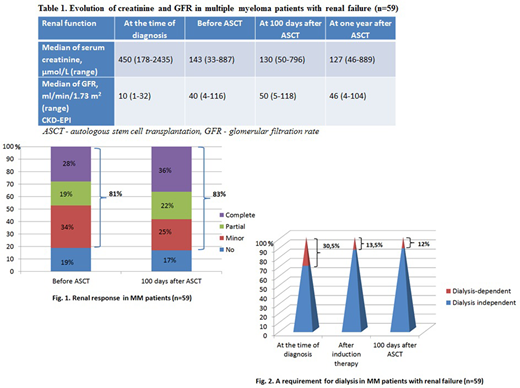
A retrospective single-center study was performed, including 59 (28 males, 31females) MM patients with renal failure at the time of diagnosis aged 19 to 65 years (median 53) underwent ASCT during a period from 2014 to 2019. Hematologic response and renal response was defined according to International Myeloma Working Group criteria. At the time of diagnosis median of serum creatinine level was 450 μmol/L, and median of glomerular filtration rate (GFR) was 10 ml/min/1.73 m2 (CKD-EPI). 18 patients (30,5%) were dialysis-dependent. Induction therapy included bortezomib-containing regimens in all patients, immunomodulatory drugs were used in 9 patients (15%). Before ASCT overall response rate (CR, VGPR, PR) was documented in 55 patients (93%), median of serum creatinine level was 143 μmol/L, median of GFR increased to 40 ml/min/1.73 m2. Renal response was achieved in 48 patients (81%), in 10 cases dialysis was stopped. 8 patients (13,5%) were dialysis-dependent at the time of ASCT. 43 patients (73%) underwent a single and 16 patients (27%) underwent a tandem ASCT (Mel 140-200 mg/m2). The analysis of such parameters as neutrophil and platelet recovery, a requirement for transfusion therapy was carried out in 2 subgroups: subgroup A - patients without dialysis at the time of ASCT (n = 51), subgroup B - dialysis-dependent patients at the time of ASCT (n = 8). Statistical analysis was done using Statistica 10. Survival curves were constructed using the Kaplan-Meier method. Frequency analysis (Fisher's test) was used.
Results
Median delay for neutrophil recovery was 14 days and 15 days for platelet recovery in subgroups A and B. Platelet concentrate transfusion was required for all patients of both subgroups in a comparable amount. In patients from subgroup B (dialysis-dependent) compared to those from subgroup A (dialysis independent) significant differences was observed in a requirement of red blood cell transfusions (100% vs 37%, p = 0.001).
There was no transplant-related mortality. At 100 days after ASCT overall response rate (CR, VGPR, PR) was achieved in 57 patients (96,6%), median of serum creatinine level was 130 μmol/L, and median of GFR was 50 ml/min/1.73 m2. Renal response was achieved in 49 patients (83%); in one case dialysis was stopped after ASCT (Fig. 1).
At one year after ASCT median of serum creatinine level was 127 μmol /L, and median of GFR was 46 ml/min/1.73 m2 (Table 1). Seven patients (12%) remained dialysis-dependent.
After a median follow-up of 36 months 5-year overall survival was 60%, and 5-year progression-free survival (PFS) was 40%. The analysis of PFS dependent on the severity of acute kidney injury demonstrated that the 5-year PFS of patients who were dialysis-dependent at the time of diagnosis did not differ from that in patients with mild and moderate renal impairment (42% vs 39%, respectively).
Conclusion
ASCT is feasible and safe method of treatment in MM patients with severe kidney injury. Dialysis-dependent patients during the early post-transplant period significantly more often require red blood cell transfusions (p = 0.001). Induction therapy followed by ASCT allowed reducing a requirement for dialysis from 30.5% at the time of diagnosis to 12% after ASCT (Fig. 2). In our study 11 of 18 MM patients (61%) became dialysis independent. Overall, this work confirmed no difference in PFS dependent on the severity of acute kidney injury; dialysis-dependent myeloma patients should not be excluded from high dose therapy followed by ASCT.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal